Big Pharma influences high-impact journals to selectively publish (purportedly) negative studies while outright rejecting positive studies from publication. JAMA did it again yesterday.
One of the main corporate disinformation tactics used to suppress “science that is inconvenient to their interests” is to employ what is called the “Diversion,” defined by the Union of Concerned Scientists as “injecting doubt or uncertainty where there is none.” JAMA just did it to ivermectin for the 2nd time in the pandemic.
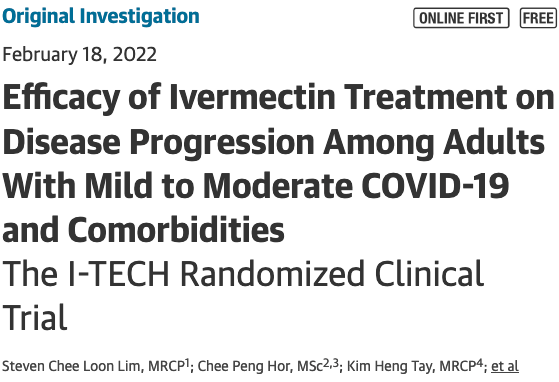
JAMA published a “negative” ivermectin study yesterday.. which immediately triggered physicians, academics, and the captured media to gleefully decry to the world, “see, I told you it doesn’t work!” As a leader of an organization that has put together highly effective treatment protocols for COVID using a combination of repurposed, generic medicines with ivermectin as one of their core components, we also immediately are attacked across the world.. in journal editorials, across major media, social media, hospital “water coolers”.. you get it.
We have lived through days like this multiple time during the pandemic, where suddenly our credibility, expertise, and advocacy are widely questioned when a high impact journal suddenly publishes a purportedly negative study on ivermectin. Such days are exhausting as many colleagues and supporters both inside and outside the organization look to us to immediately rebut these newfound and false assertions. I have written many rebuttals, (white papers) to the NIH, EMA, and the WHO each time their faulty, biased, and oftentimes outright corrupt non-recommendations for ivermectin are issued over such single trials. Over a hundred doctors published a rebuttal attack the last time JAMA did this.
I guess this time I will just briefly go it alone.
There are really three main problems with this study and its aftermath;
1) Publication Bias: given my personal knowledge of a number of researchers whose profoundly positive ivermectin studies were rejected by JAMA, they, for the second time in a row, reveal a profound publication bias. It is a well-known disinformation tactic for high impact journals like JAMA to somehow only publish studies without “statistically significant benefits” for medicines that Pharma does not want to see in play (generally generic medcines), as they similarly avoid publishing studies of “hrams” assciated with Pharma favored products (i.e tobacco studies last century and/or vaccine studies this one). What is fascinating is that JAMA’s (“PHAMA’s”) ivermectin papers actually all report important benefits.. but most importantly for JAMA, none that reach “statistical significance.”
2) Study Conclusion: JAMA saw fit to ensure inclusion of this phrase at the end of the conclusion, “the findings do not support the use of ivermectin for treatment of mild COVID-19,” despite what could arguably be called a compellingly supportive study based on a number of important, near statistically significant reductions in secondary outcomes like death. Instead, per their strict criteria, conclusion statements consistently avoid mention of large differences in massively important secondary outcomes. Best example of this behavior by JAMA was the IV Vitamin C in ARDS trial. Read the conclusion. Then read the paper, and look at Table 2 and Figure 3… you find a massive, statistically significant reduction in mortality in those treated with IV Vitamin C. Hard to find.. but it is there. If JAMA wouldn’t allow those authors to mention it in that paper’s abstract conclusion, no surprise they did it again here.
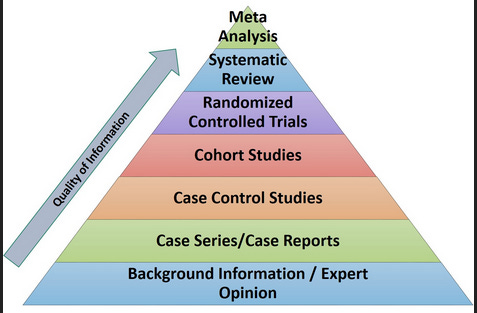
3) the masses of doctors and media who simply propagate and disseminate that sentence and abstract .. without reading the actual study or reviewing the actual data while ignorant of the findings from the highest level of medical evidence.. the “meta-analyses” of ivermectin (summary analyses of all trials).
The way that sentence was written and where it was placed and in what journal it appeared was.. highly strategic (and very effective) as the entities who have been trying to suppress and distort the evidence of efficacy of ivermectin know exactly how to further stoke the smug arrogance and trigger the “I told you so’s” from all those doctors with propagandized, deeply ignorant bias against ivermectin, a proportion which likely includes well over 90% of academic physicians.
Although the above attack strategy on ivermectin is effective, to most of “us” it is really easy to see how crazily the conclusion departs from not only the study’s own data, but the totality of the published evidence (and every single “comprehensive” meta-analysis) which all show repeatedly shorter times to viral clearance, clinical recovery, fewer hospitalizations, and far less death when COVID patients are treated with ivermectin.
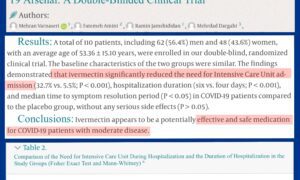
All you have to do is read the study to understand a few simple things, namely that the primary outcome was not patient-centered (need for oxygen while in hospital?), while the “important” patient centered outcomes were “secondary” ones (death and need for mechanical ventialtion), and although these two events happened so few times that a statistically significant result was near impossible to achieve.. the differences they found came very, very close to statistical significance! The ”p” value (probability the findings were due to chance) for the mortality reduction in IVM treated patients (the control groups deaths were over 3X as much as the ivermectin group) was… 0.09! Statistical significance is generally accepted (but often debated!) as a p value less than 0.05, meaning that there must be less than a 5 percent probability that the study findings were “due to chance.” In this study there was a 9% probability that the differences were due to chance. Conversely, this means that there was a 91% probability that the difference in death was REAL and reproducible. Note the p value for the need for mechanical ventilation was also quite low despite so few events observed, p = 0.17.
Find me one patient who wouldn’t take those odds while ill in a hospital with COVID with a drug as ridiculously safe as ivermectin. My god. Find me one patient who would worry about developing a need for oxygen more than developing a condition called death.
The reason why I say the standard p value of .05 is often debated is that many scientists and physicians like myself feel strongly that lower p values should be required only when the drug is either high risk, high cost, novel or other data are few. Further, many of us also recognize that over-relying on p values leads to critical signals of efficacy being ignored, especially when event rates are low. Ivermectin has incredible safety and low cost, with, as mentioned above, a massively positive data signal from 78 controlled trials and numerous health ministry treatment programs around the world. A 91% chance that the massive reduction in death they found was real and repeatable with ivermectin should convince almost anyone to want to take ivermectin if ill with COVID. Summary (meta-analysis) data of ALL trials actually represent the highest and strongest form of medical evidence.. not just one trial.
Yet the obsessiveness with p values of a single study in modern, “evidence based medicine” (I call it evidence based maniacisim (EBM) is literally killing people. And that is why one of the most popular scientific papers in the last decade is a paper in Nature called “Scientists Rise Up Against Statistical Significance.” I wish every doctor would read (and understand) the deep meaning and massive implications of what that paper teaches those of us in the medical sciences whose patients fate is often in our hands.. rather than the overly stringent p values the EBManiacs demand. Docs will literallly let someone die if a study of a medicine that found an important benefit does not have an associated p value of less than .05. When it is .09 and a secondary outcome? Too arbitrary, not rigorous enough to use the medicine, even in the dying. Even if it is the safest, most benign, and lowest cost medicine in the world. Now do you understand why I have effectively left institutionalized medicine?
Now just look at the headlines generated from the way that abstract was worded shall we? (Numerous examples)


Now you know why the obsessive academic EBM’ers and their misused p values lead the idiotic media into a frenzy.. and people die as a result?
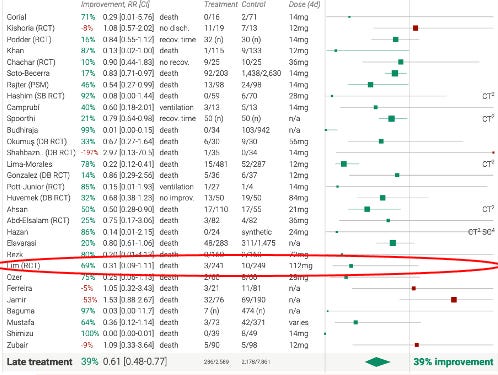
Science writers and reporters (and physicians) should know that a single study is not how we draw conclusions on the efficacy of a medicine given that the most sound conclusions are drawn from summary data from ALL the trials of ivermectin. This study, contrary to the headlines, actually strengthens the already existing, and statistically significant summary data of ivermectin’s effect on mechanical ventilation and death. Period. With now 78 controlled study results including over 85,000 patients, numerous successful health ministry reports of ivermectin early treatment programs, and powerful, positive meta-analyses, I will argue with anyone at anytime, that ivermectin has one of the most profoundly positive summary evidence bases of almost any medicine in history. And this study does nothing but further strengthen that signal. Look at how it shows up on the existing Forest plot of just the late treatment trials (the early treatment trials show double the efficacy of the below). It actually strengthens the signal for mortality reduction. How ‘s that for a headline?
Now you know why this supposed debate is so exhausting. Dealing with the combination of profound ignorance paired with such deep and willful bias of those who have already staked their reputations, credibility, and most importantly, their anti-ivermectin recommendations and policies on studies like this appear fruitless.
The absurdity of this behavior was so well pointed out by Dr. Mobeen Syed (drbeen.com) in his review of the study when he contrasted this study’s conclusion with the medical evidence used in support of the FDA’s EUA for Bebtelovimab last week (February 11th, 2022):
“the rates of COVID-19 related hospitalization and death seen in in those who received bebtelovimab alone or with other monoclonal antibodies were generally lower than the placebo rate reported in prior trials of other monoclonal antibodies in high risk patients. Conclusions are limited as these data are from different trials when different viral variants were circulating and baseline risk factors varied.”
“Generally lower”..means the differences were clearly NOT statistically significant.. or they would have said so. And the placebo comparisons they are using are just laughable. No-one ever could get away with such nonsense comparisons to other products in other variants. Absurd.
He also points out that in published reviews of remdesivir, non-statistically significant results actually led to allowing published conclusions of “mortality was lower.” Whatever.
So can we agree that, since the FDA is OK with using such a non-statistically significant impact on highly important outcomes such as hospitalization and death to issue an EUA for a product with significant risks, we all should be OK with the similar finding of “generally lower” rates of mechanical ventilation and death reported in this study? Again, I leave you with the below Forest Plot – notice the circled medicines are the ONLY ones recommended by the US health agencies. And notice their profit potential compared to all the others. The war on repurposed drugs continues apace.

P.S. I just want to say how much I appreciate all the subscribers to my substack, and especially the paid ones! Your support is so greatly appreciated. Thanks my friends.
Recommended for you