We are currently experiencing a period of apparent Covid silence. In many countries, hospitalization and mortality rates due to Covid-19 (C-19) are relatively low (i.e., compared to those recorded at the end of 2022), and in several countries where they were recently slightly rising, we now observe a systematic decrease. Moreover, this trend often coincides with a decrease in the detection of SARS-CoV-2 in wastewater, although wastewater viral activity levels remain very high in some countries/ states. All of this is certainly not the result of renewed vaccination campaigns in autumn 2023, given that the vaccination rate was particularly low.
In my humble opinion, the aforementioned decrease reflects the vigorous uptake of the virus by antigen-presenting cells in C-19 vaccinated individuals. This leads to a strong activation of cytolytic T lymphocytes (CTLs). It is precisely these CTLs that destroy virus-infected cells, thereby not only curbing virus shedding but also increasingly restraining disease caused by the virus. When enhanced CTL activation becomes widespread in a highly C-19 vaccinated population, it is, of course, not conducive to the spread of the virus. Nevertheless, we must not forget that this does not prevent the virus from continuing to spread. The circulating strains (especially JN.1, i.e., BA2.86.1.1, and its derivatives) are highly infectious and, due to the lack of noteworthy clinical symptoms, are often transmitted asymptomatically. In other words, they have the chance to continue multiplying and generating variants, from which those are selected that best resist the negative influence of CTLs on virus transmission.
Where, on the one hand, more asymptomatic SARS-CoV-2 infections occur, we also observe an increased incidence of illness due to other respiratory viruses (e.g., RSV, Influenza), as well as a further rise in the number of cases of cancer and chronic infectious diseases. As previously indicated, I believe this is related to the fact that the activated, MHC class I-unrestricted CTLs in C-19 vaccinees are also effective against host cells infected with other respiratory viruses, thereby enabling asymptomatic transmission and causing disease in individuals lacking immune protection against these viruses. Additionally, the strong activation of antigen-presenting cells in C-19 vaccinees leads to the suppression of T cell-mediated immunity that normally controls cancers and underlying chronic infections (via the PD [Programmed death]-1/PD-L[igand]1 pathway). Consequently, we are currently facing a situation where both C-19-associated and vaccine-induced, non-C-19-associated diseases can occur in highly C-19 vaccinated populations. I believe that this marks the transition to a situation where vaccine breakthrough infections will eventually cause enhanced severe C-19 disease and dominate the symptomatology in highly C-19 vaccinated countries.
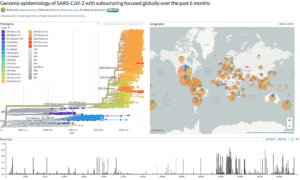
JN.1 has, in the meantime, differentiated into additional descendants distinguished by several mutations that do not immediately result in an increase in the intrinsic infectivity of the virus, which is already exceptionally high. It is evident that the relentless spread and mutations of the virus will not be curbed by so-called hybrid immunity. While the JN.1 clan comprises the most prominent variants globally, neither JN.1 nor its derivatives appear to induce more severe outcomes than previous SARS-CoV-2 lineages. Moreover, C-19 infections are causing severe disease less frequently than earlier in the pandemic.
Hybrid immunity related to the alleged protection from the combination of both vaccination and infection is considered ‘the best of both worlds’ by those who don’t understand the ongoing dynamics of the adaptive immune response in C-19 vaccinees (https://pubmed.ncbi.nlm.nih.gov/37592872/). As they don’t grasp the concept of mRNA- or VBTI (vaccine breakthrough infection)-induced immune refocusing, several so-called experts believe that hybrid immunity is superior in magnitude and durability to that provided by either vaccine immunity or natural immunity alone. Some of them go even further, claiming that hybrid immunity has enabled herd immunity and that, as a result, the virus has become endemic!
I simply cannot comprehend how scientists conducting research on this pandemic can spout such nonsense.
In any case, there seems to be a consensus among scientists that the evolution of this virus is unpredictable and continues to be so, and an increasing number of dedicated mutation spotters are now clearly stating that a higher infection rate of the virus by no means implies a reduction in virulence.
Dr. Rob Rennebohm compares the ongoing changes in the host’s immune response to the adaptive strategies employed by an army that, when losing a battle, shifts to alternative tactics (https://www.voiceforscienceandsolidarity.org/scientific-blog/an-armed-forces-analogy-the-immunologic-consequences-of-the-covid-19-mass-vaccination-campaign). Using this parallel, he succinctly explains why I am convinced that the ongoing evolution of this (immune escape!) pandemic will, in fact, have the opposite effect. Although the immune pressure exerted by highly C-19 vaccinated populations will significantly reduce viral transmission from one host to another, it won’t be able to prevent strong spread within the same host. This aligns precisely with the characteristics of high virulence.
Whether one believes in my theory or not, the fact remains that, even purely theoretically, it can go both ways. Considering that people are no longer enthusiastic about receiving additional shots and that, at this stage of the pandemic, even updated booster vaccinations fail to generate significant neutralizing antibodies, one must wonder how such a passive stance from our health authorities is tolerated.
It only demonstrates how much the people have become worn out and exhausted by the mismanagement of this crisis over the past years and all the nonsense spouted by the so-called Corona experts. While I perfectly understand this indifference, I am not hiding my scientifically grounded fear of the potential consequences that an entirely new type of SARS-CoV-2 variant could cause in highly C-19 vaccinated populations. Therefore, I continue to assert that “Society in highly C-19 vaccinated countries will be caught by surprise.” It is very difficult, though, to predict when the expected metamorphosis of the virus will occur. The emergence of a highly infectious Omicron generation did not take long after Delta. Now the only question is how long the virus will need to conjure up a variant that will allow it to eventually escape the life-threatening immune pressure it is currently undergoing. In any case, Dr. Rob Rennebohm once again provides guidance here and also explains why timely treatment with ivermectin makes perfect sense (https://notesfromthesocialclinic.org/wp-content/uploads/2024/01/COVID-ANALYSIS-232g-IVERMECTIN-SUMMARY.pdf).
Recommended for you